How to read HeadCT
January 9, 2021
This blogs talks about how to read head ct scans and how to identify different types of bleeds.
Introduction
Head CT is also called Brain CT. It refers to computed tomography examination of the brain and surrounding structures. It can be performed in 2 ways:
- Non-Contrast Study
- Contrast Study
Preparation:
Without Contrast: No preparation is required.
With Contrast:
- Only one CT contrast study should be scheduled within a 48 hour period.
- BUN & Creatinine must be done within 72 hours of the scan.
- Nothing but clear liquid after midnight before the scan.
- NPO 4 hours prior to exam (no food or drink).
During examination of CT scans, it is important to review old scans as they may provide information which is as clinically important as the current scans
For example:
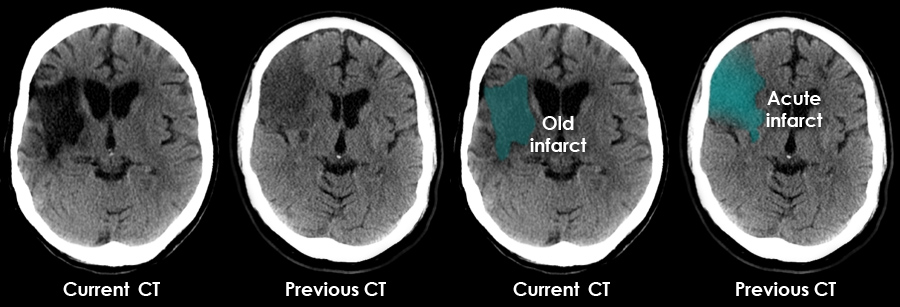
This elderly patient - who presented with acute confusion - has a large area of low density in the right frontal lobe seen on the current CT Review of a previous CT revealed that the abnormality in the brain was not new, but related to an infarct which occurred 5 months earlier The current CT appearances were not the cause of the acute confusion (urinary tract infection in this case)
Approach
In emergency situations radiologists tend to follow this mnemonic: Blood Can Be Very Bad (BCBVB).
B: blood
look for epidural hematoma, subdural hematoma, intraparenchymal hemorrhage, intraventricular hemorrhage, subarachnoid hemorrhage and (also) extracranial hemorrhage
C: cisterns
look for the presence of blood, effacement and asymmetry in four key cisterns (perimesencephalic, suprasellar, quadrigeminal and Sylvian cisterns)
B: brain
look for asymmetry or effacement of the sulcal pattern, gray-white matter differentiation (including the insular ribbon sign), structural shifts and abnormal hypodensities (e.g. air, edema, fat) or hyperdensities (e.g. blood, calcification)
V: ventricles
look for intraventricular hemorrhage, ventricular effacement or shift and for hydrocephalus
B: bone
look for skull fractures (especially basal) on bone windows (soft tissue swelling, mastoid air cells and paranasal sinuses fluid in the setting of trauma should raise the possibility of a skull fracture; intracranial air means that the skull and the dura have been violated somewhere)
To look for these neuropathology, there is a 3 step process:

For this blog, we focus on bleeds/hemorrhage and its subtypes.
The following points can be used as a guide to assess a brain CT to demonstrate/exclude a hemorrhage.
Brain parenchyma
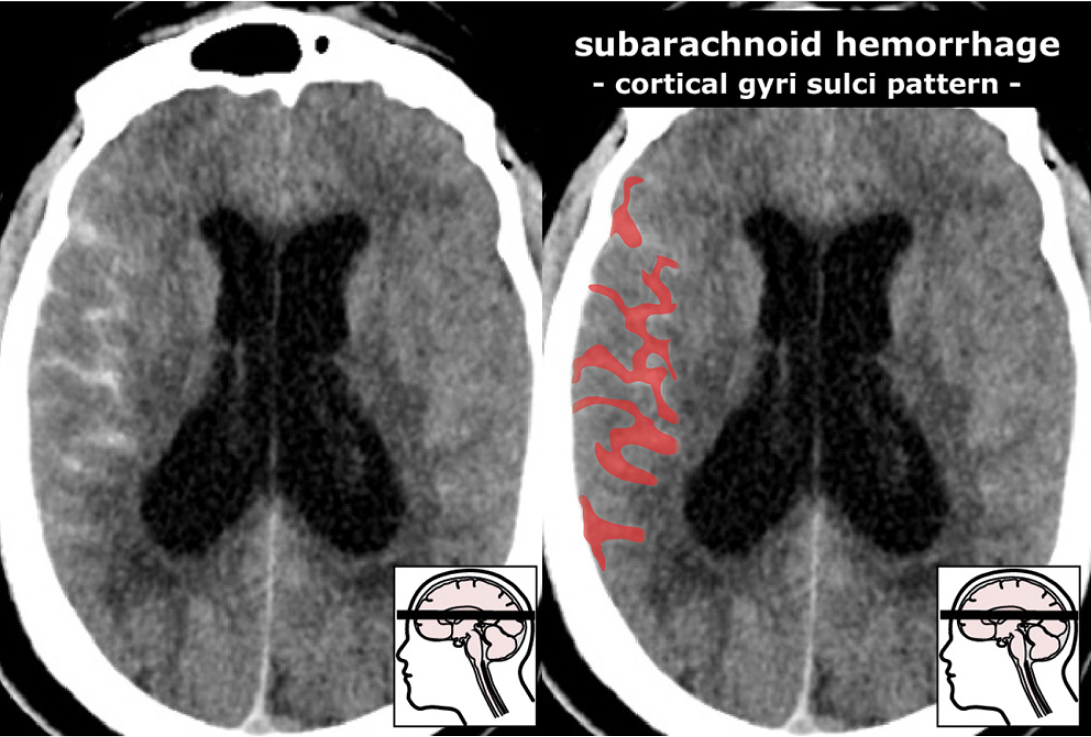
- is there asymmetry anywhere or obliteration of the gyri sulci pattern?
- abnormal gray-white matter differentiation?
- hypo/hyperdense abnormalities?
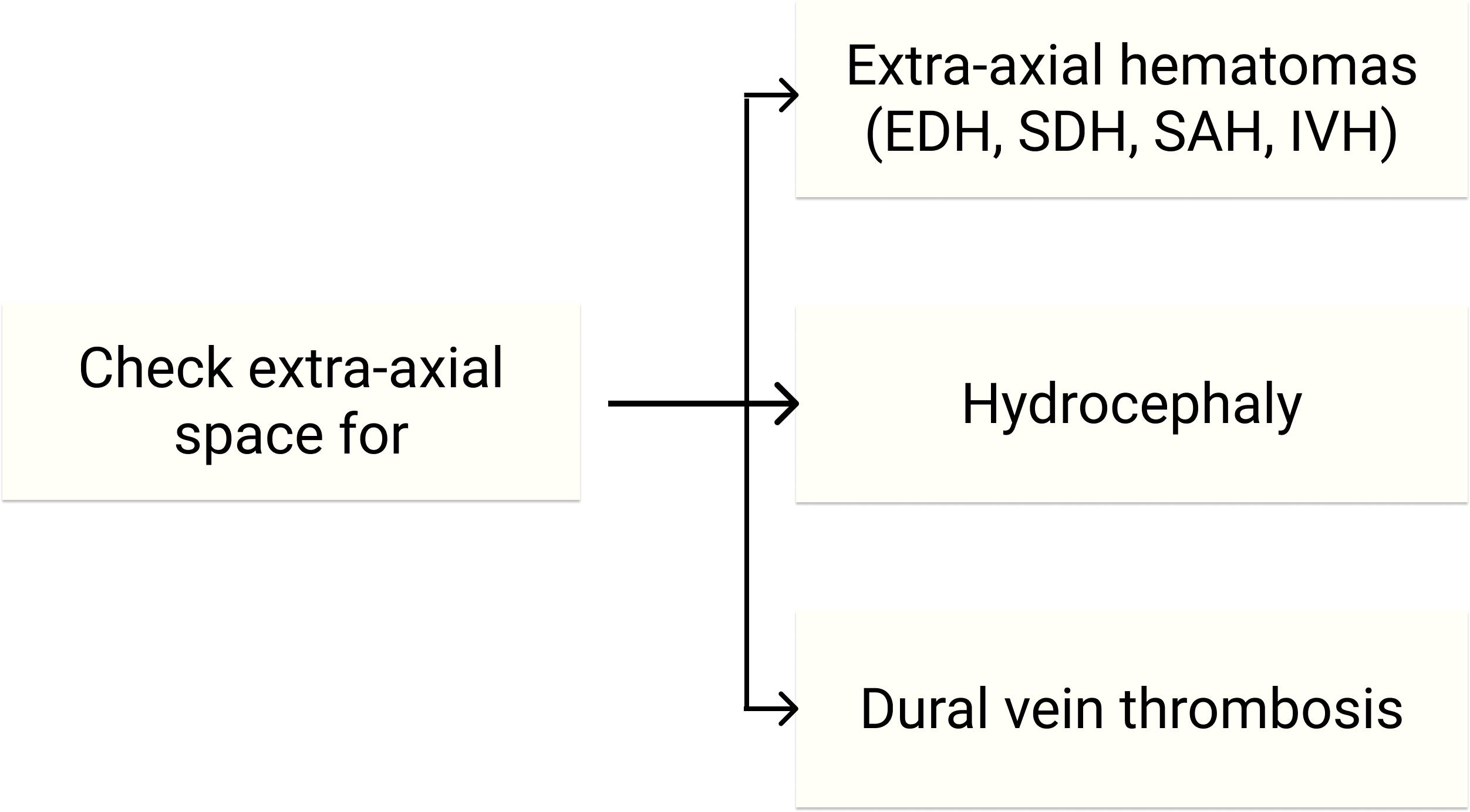
Hemorrhage
- type/cause/location?
- subarachnoid cisterns; obliteration of the W shape, pentagon, moon shape, Sylvian fissure?
- mass effect or signs of herniation? is there still space around the brain stem?
Ventricular system
- hydrocephalus?
- intraventricular blood?
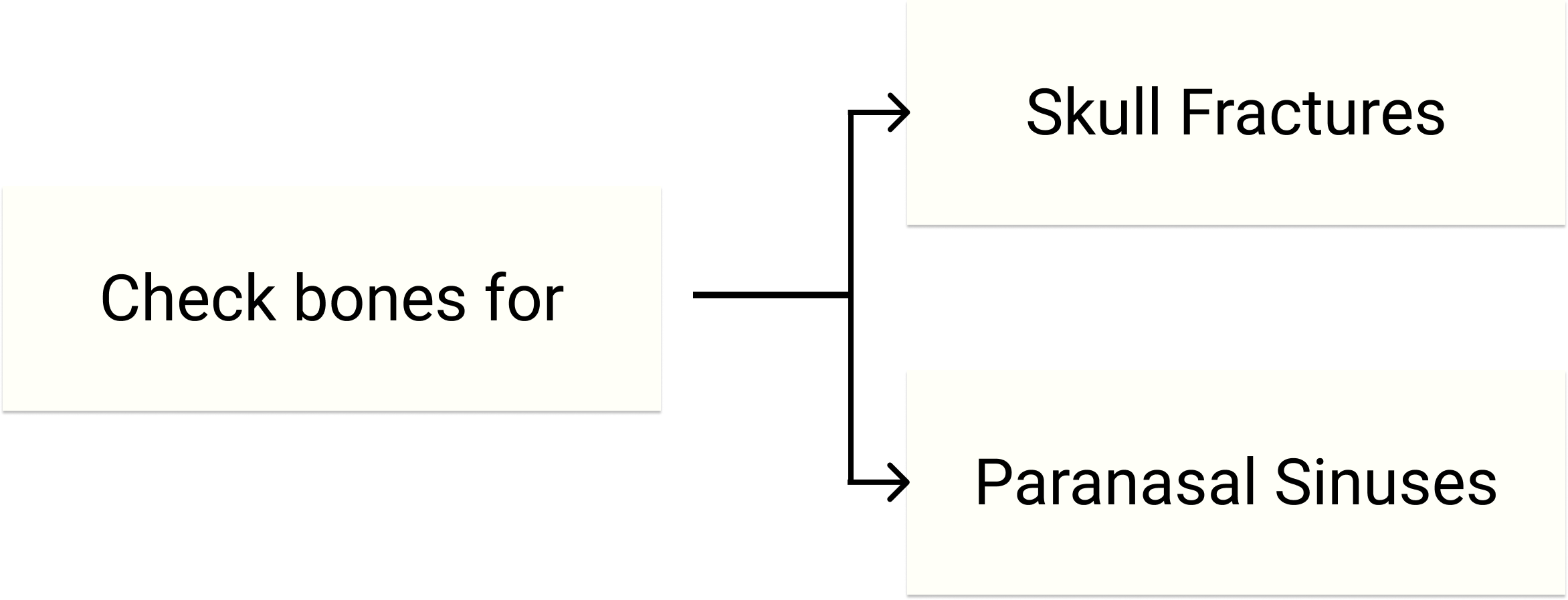
Bone
- extracranial soft tissue swelling?
- fracture? Pneumocephalus?
- normal air content of the sinuses and the mastoid? Air-fluid (blood) levels in the sinus? (CAUTION: fracture!)
Old examinations
- new findings?
Hemorrhage Categorization
When a blood vessel within the skull is ruptured or leaks, it is called Intracranial hemorrhage (ICH)
ICH encompasses many conditions characterized by the extravascular accumulation of blood within different intracranial spaces. Following categorization is based on locaiton:
Intra-axial hemorrhage is bleeding within the brain itself, or cerebral hemorrhage. This category includes intraparenchymal hemorrhage (bleeding within the brain tissue) and intraventricular hemorrhage (bleeding within the brain’s ventricles).
Subtypes:
intracerebral hemorrhage
- lobar hemorrhage
- hypertensive hemorrhage
- basal ganglia hemorrhage
- pontine hemorrhage
- cerebellar hemorrhage
Intracerebral hemorrhage also called intraparenchymal cerebral hemorrhage, is a subset of an intracranial hemorrhage. It is the acute accumulation of blood within the parenchyma (tissues) of the brain.
Extra-axial hemorrhage, bleeding that occurs within the skull but outside of the brain tissue, falls into three subtypes: Epidural hemorrhage (extradural hemorrhage) which occur between the dura mater (the outermost meninx) and the skull, is caused by trauma.
Subtypes:
- extradural hemorrhage (EDH)
- intralaminar dural hemorrhage
- subdural hemorrhage (SDH)
- subarachnoid hemorrhage (SAH)
- intraventricular hemorrhage (IVH)
- subpial hemorrhage
Lets look at above mentioned neuropathology based on 3 steps metioned in Introduction:
Brain Parenchyma
Intra-axial hemorrhages
Lobar hemorrhage
Location : Lobar -> Lobes
Hyperdense collection of blood, located superficially within the lobes of the brain (i.e. not in the basal ganglia).
They are usually large and more common in elderly patients.

Extension into the subdural or subarachnoid and even intraventricular(common to basal ganglia hemorrhage - hypertensive) space may be seen.
Hypertensive hemorrhage
Distribution that matches incidence of hypertensive hemorrhages:
- 80% around basal ganglia
- 10% pons
- 10% cerebellum
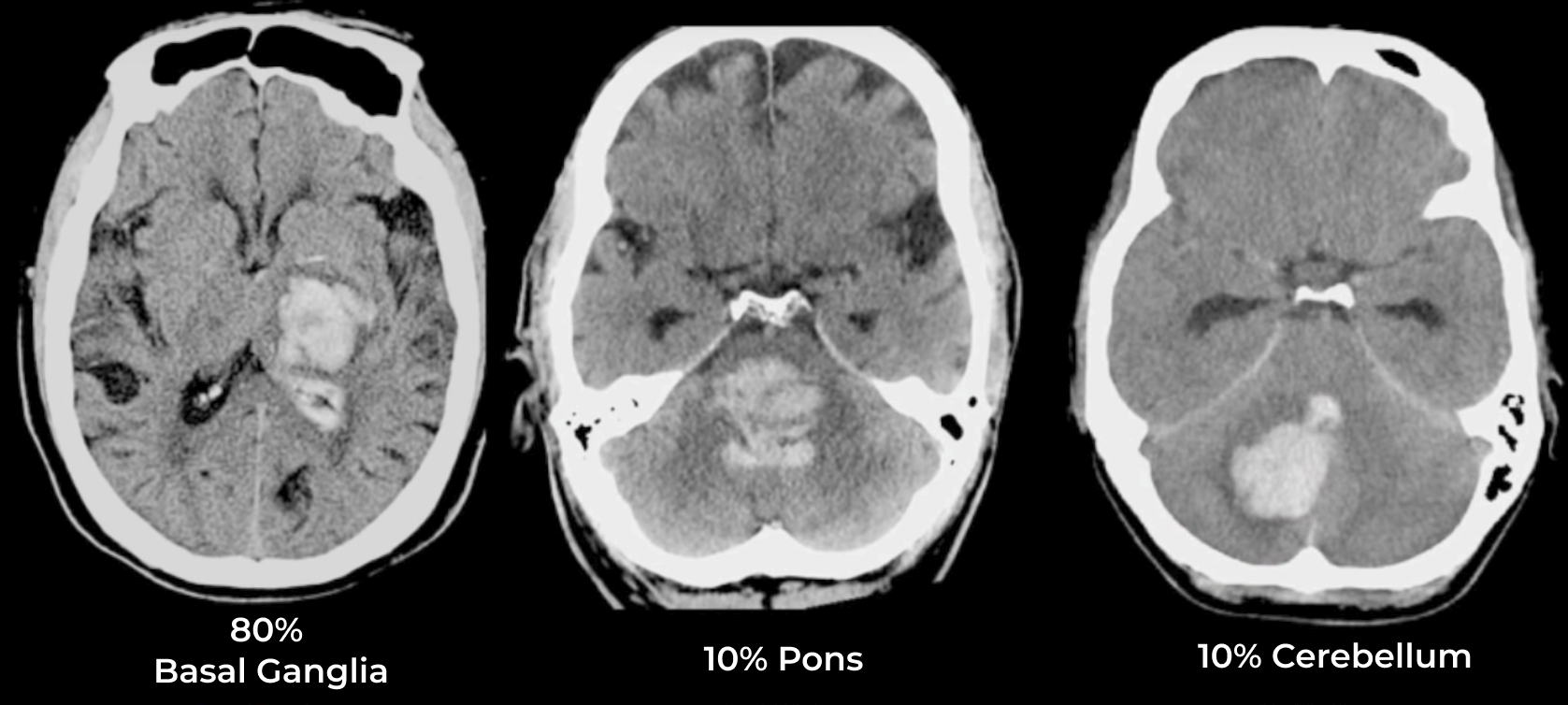
1- Basal ganglia hemorrhage
Name pretty much gives away the location of hemorrhage: around basal ganglia.
Abnormal Hyperdensity centered on the basal ganglia or thalamus. It will be characterized as intraparenchymal hemorrhage.
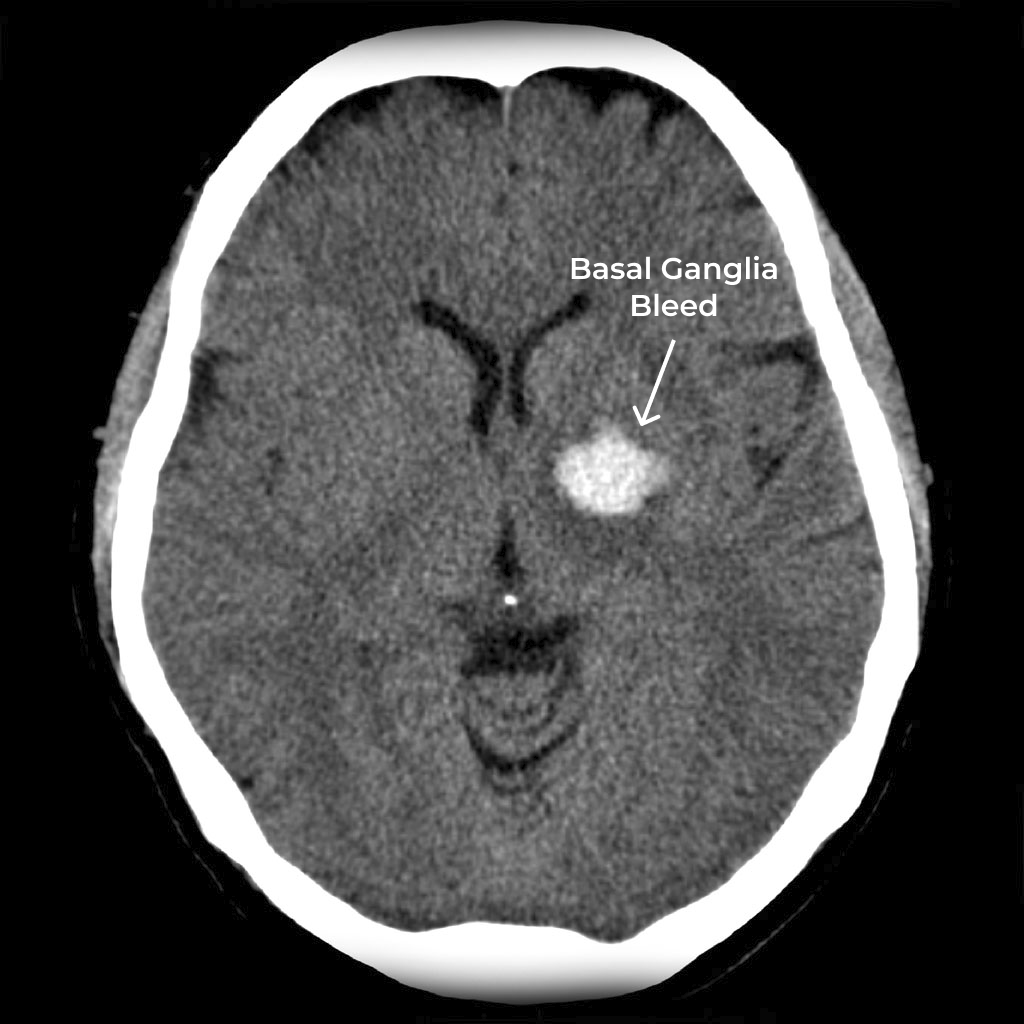
Often times there may be an intraventricular extension. In this case it also becomes intraventricular hemorrhage.

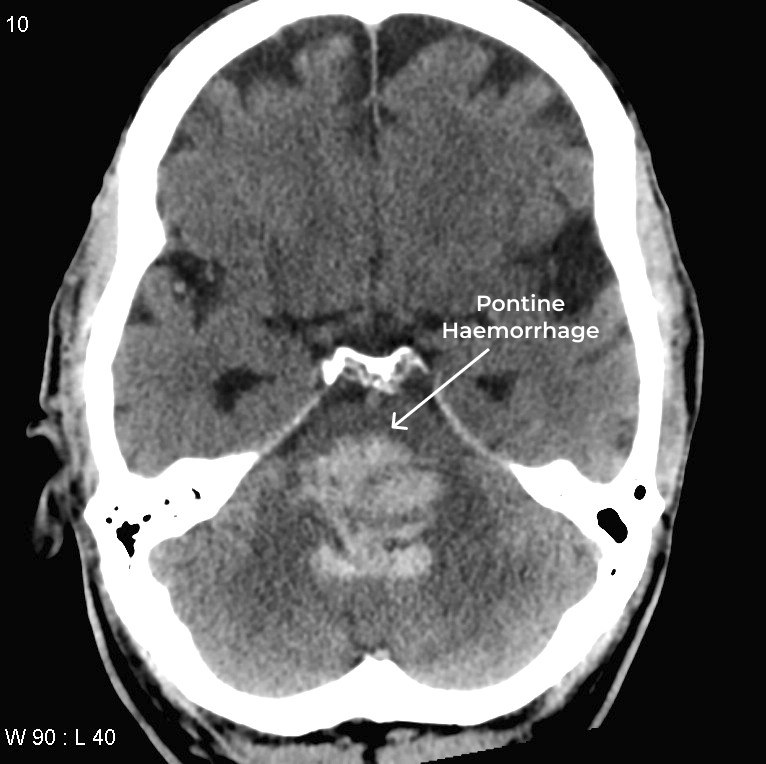
2- Pontine hemorrhage
location: pontine -> pons
These bleeds frequently rupture into the 4th ventricle as shown in figure.
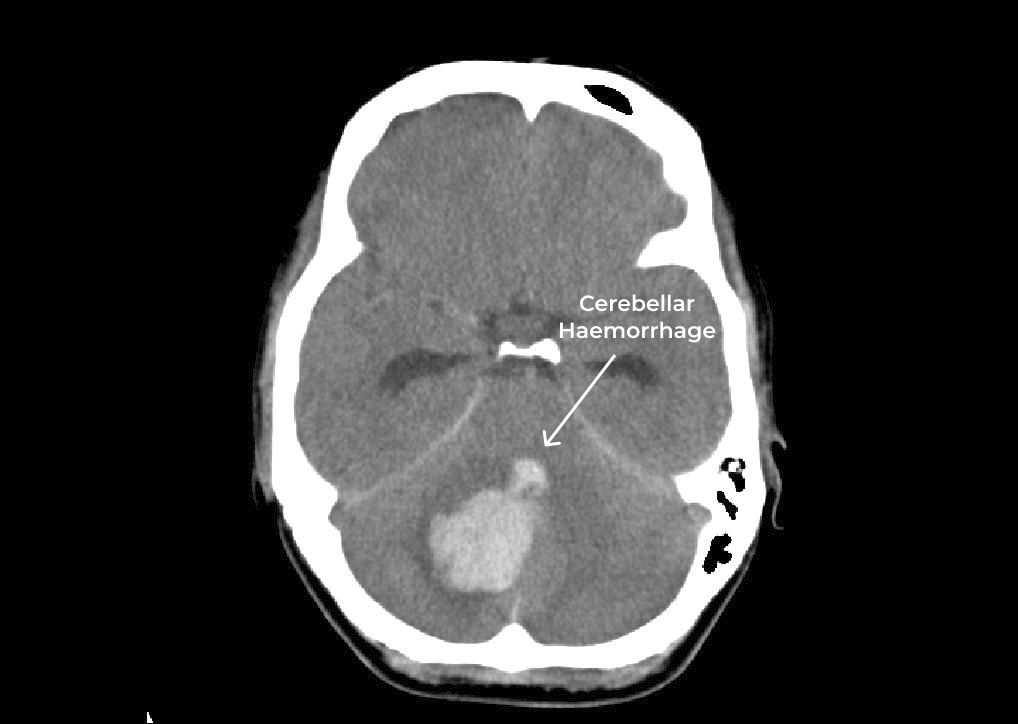
3- Cerebellar hemorrhage
location: cerebellar hemispheres
It appears as hyperdensity within the cerebellar hemispheres. Extension into the fourth ventricle or subarachnoid space is relatively common.
Outside Brain Parenchyma
Extra-axial hemorrhage
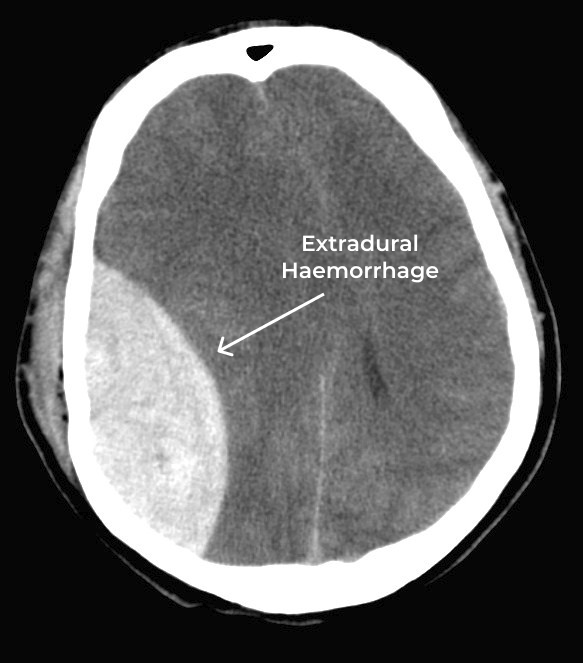
Extradural hemorrhage
location: between the inner surface of the skull and outer layer of the dura
shape: bi-convex (or lentiform)
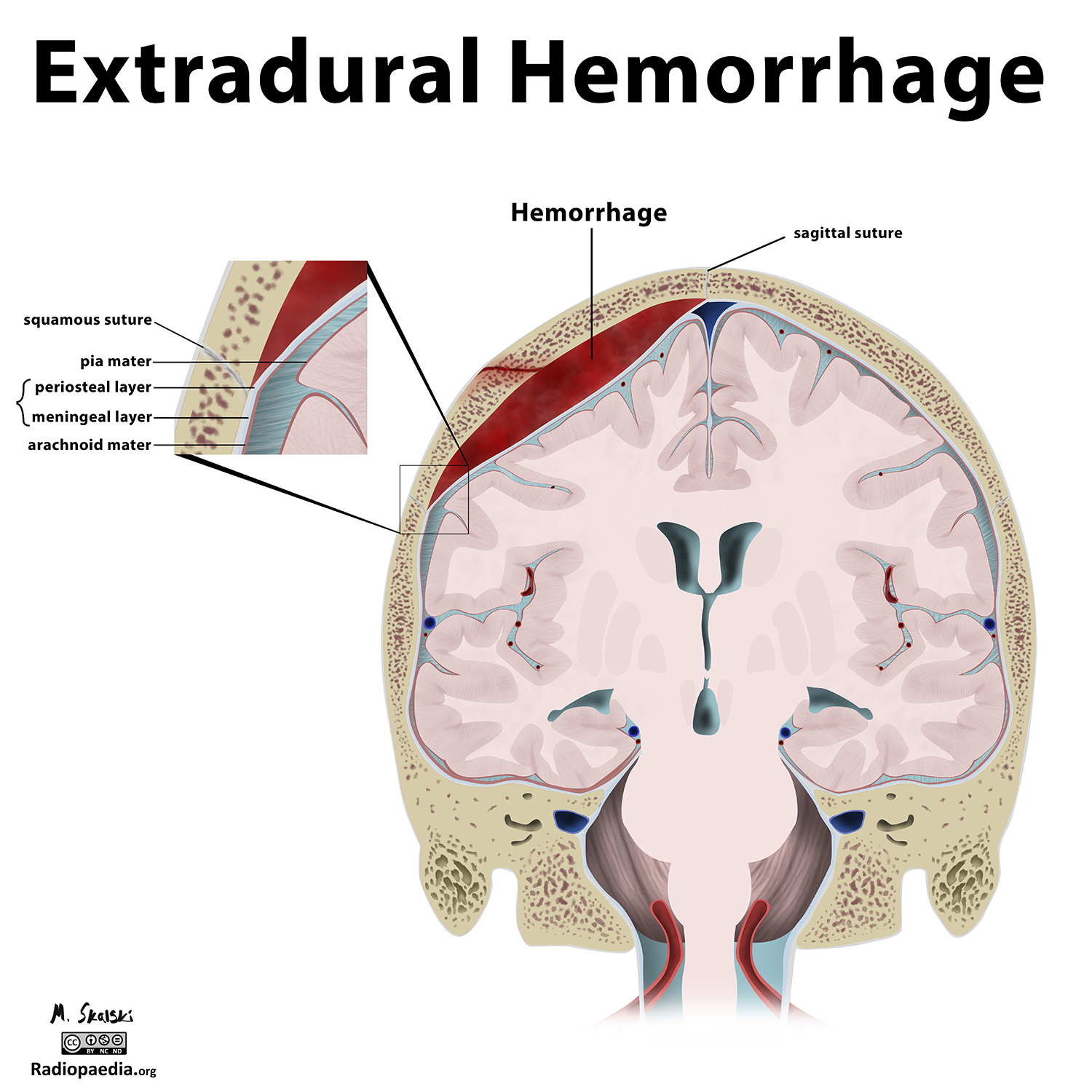
Extradural hematoma (EDH), also known as an epidural hematoma.
EDHs are hyperdense. Depending on their size, secondary features of mass effect (e.g. midline shift, subfalcine herniation, uncal herniation) may be present.
Intralaminar dural hemorrhage
location: between the two layers of the dura mater
Intralaminar dural hematomas in the intracranial space, are exceedingly rare.
Subdural hemorrhage
location: between the dura and arachnoid mater of the meninges around the brain
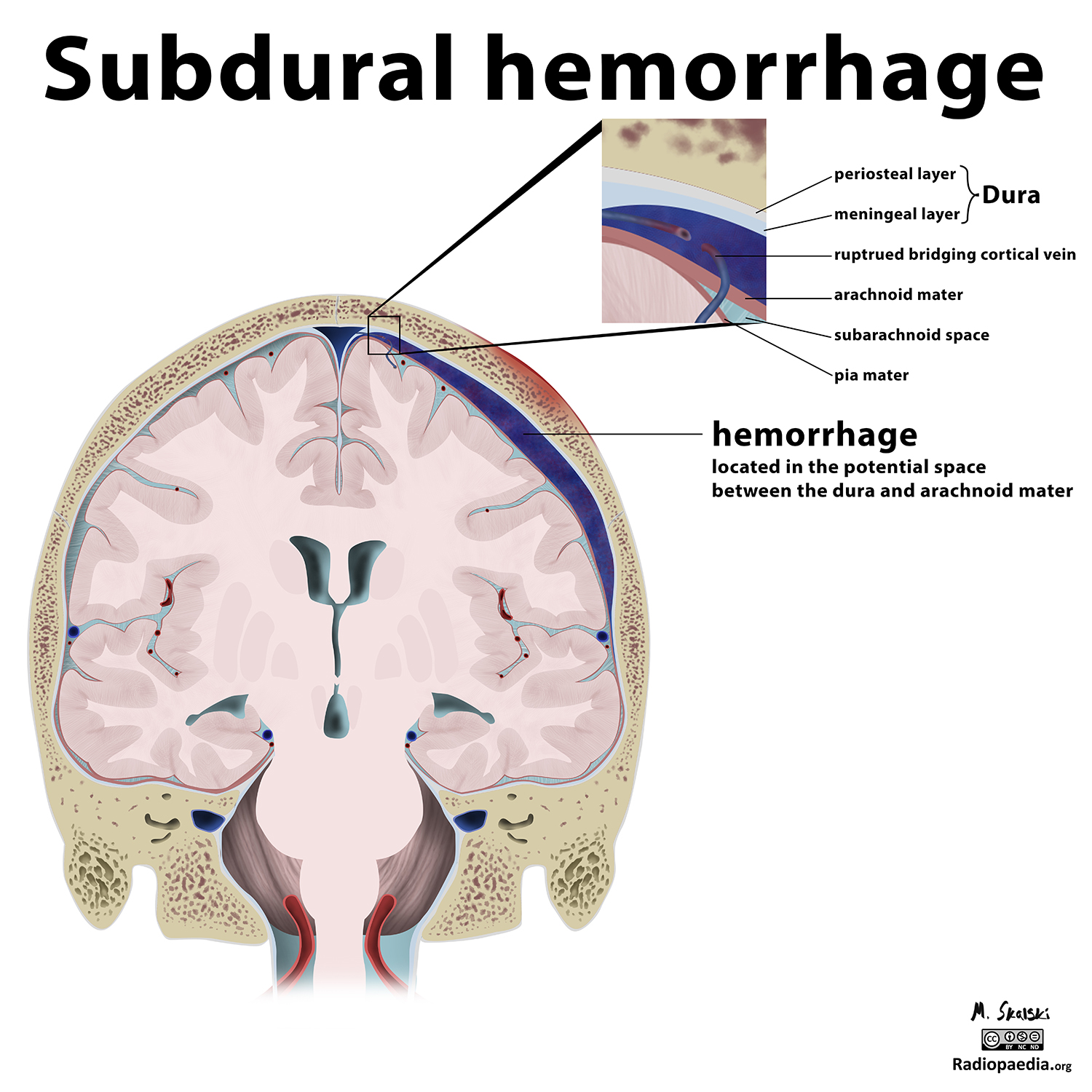
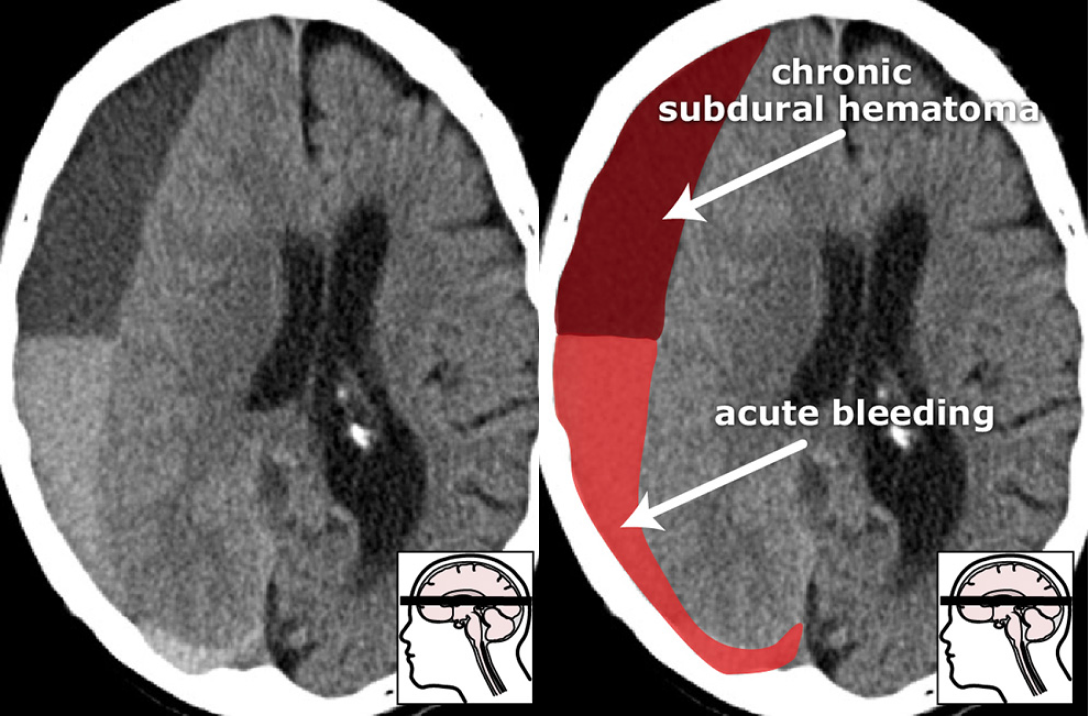
The aspect of a Subdural hemorrhage (SDH) on a CT may vary: from hyperdense/heterogeneous in the acute phase to iso/hypodense during the chronic phase. In a mixed picture, fresh hemorrhages are seen in a chronic subdural hematoma.
Hyperacute
appearance: relatively isodense (same density) to cortex with swirled appearance.
mass-effect: cerebral swelling accentuates the mass-effect created by the collection of the clot, serum and ongoing unclotted blood.
Acute
shape: crescent-shaped
appearance: hyperdense relative to the cortex
Subacute
duration: takes 3-21 days
appearance: isodense to the adjacent cortex
Isodense appearance makes it hard to detect
key-id’s : mass-effect, thickening of cortex, CSF-filled sulci do not reach the skull but rather fade out into the subdural.
Chronic
duration: ~3 weeks
shape: crescentic shape may change to a biconvex
appearance: hypodense
Please refer to ct scans for all above stages here.
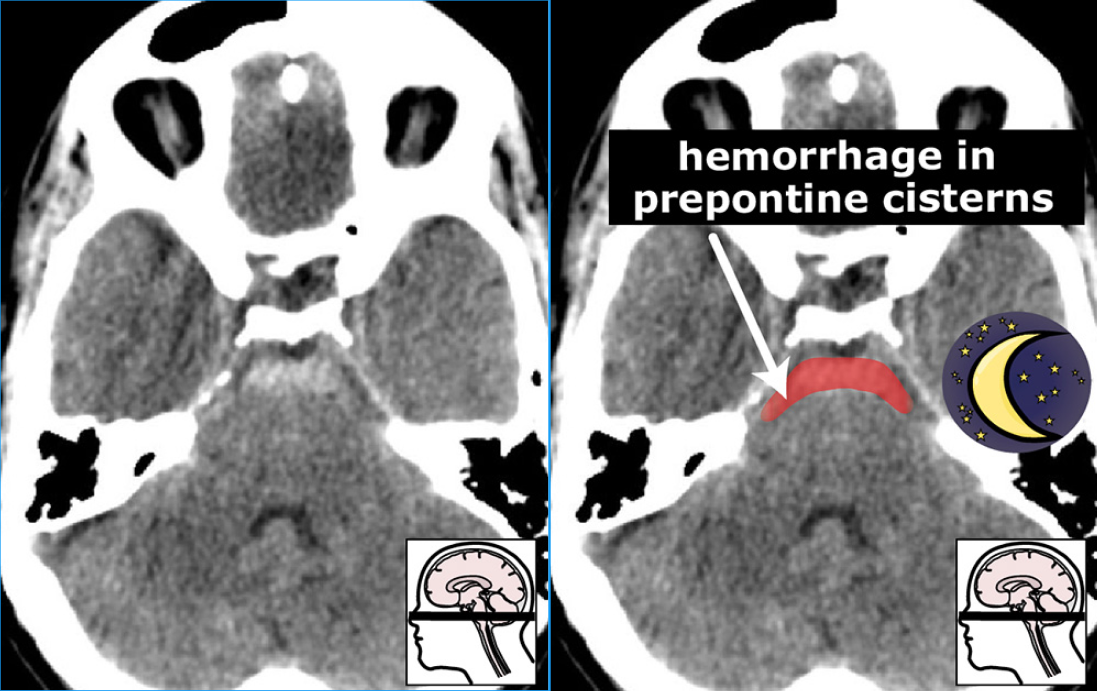
Subarachnoid hemorrhage (SAH)
location: subarachnoid spaces
The subarachnoid spaces include the basal cisterns (= space around the brain stem), the Sylvian fissure, the cerebral sulci, the intraventricular space and the interhemispheric fissure
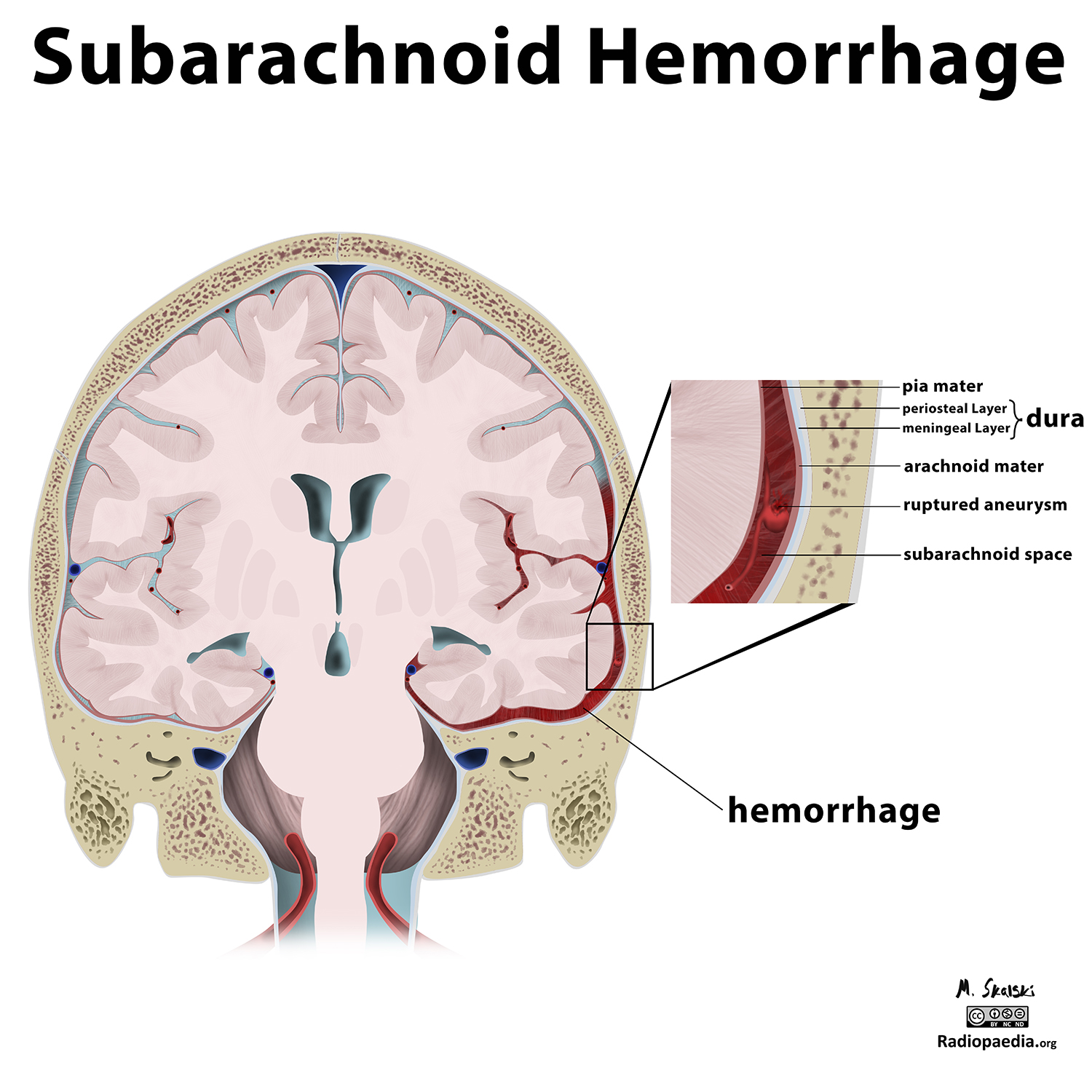
Small amounts of blood can sometimes be appreciated pooling in the interpeduncular fossa, appearing as a small hyperdense triangle, or within the occipital horns of the lateral ventricles.
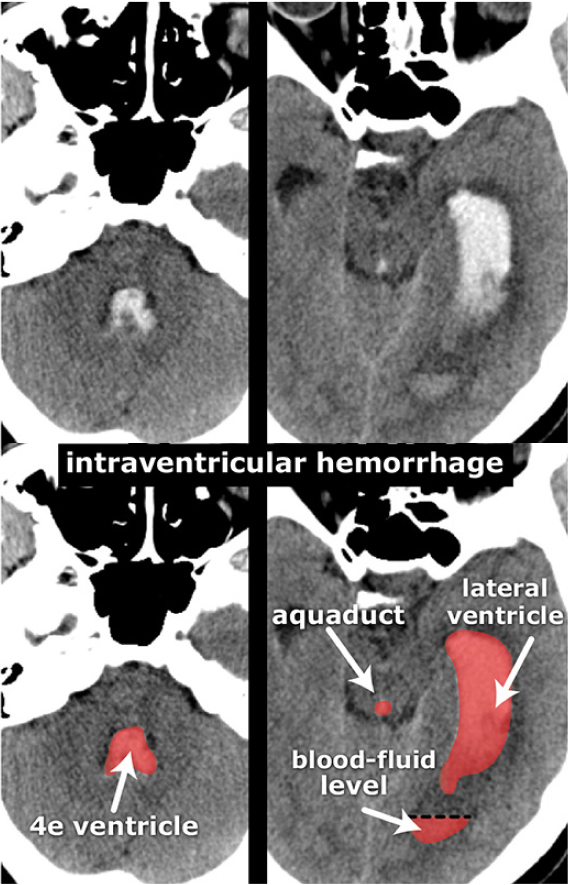
Intraventricular hemorrhage
Intraventricular hemorrhage (IVH) denotes the presence of blood within the cerebral ventricular system.
IVH is divided in 2 types: \(P(primary) < P(secondary) \rightarrow\) P being probablity
- Primary - blood in the ventricles with little (if any) parenchymal blood
- Secondary - a large extraventricular component is present (e.g. parenchymal or subarachnoid) with secondary extension into the ventricles
In above sections on hypertensive hemorrhage and subarachnoid hemorrhage, IVH CT scan is shown.
Subpial hemorrhage
location: between the cortical surface and the pia mater
Difficult to distinguish from subarachnoid hemorrhage.
It is very rare type of extra-axial intracranial hemorrhage.
Cerebral hemorrhagic contusion
location: in the frontal lobes adjacent to the floor of the anterior cranial fossa and in the temporal poles.
appearance: hyperdense foci
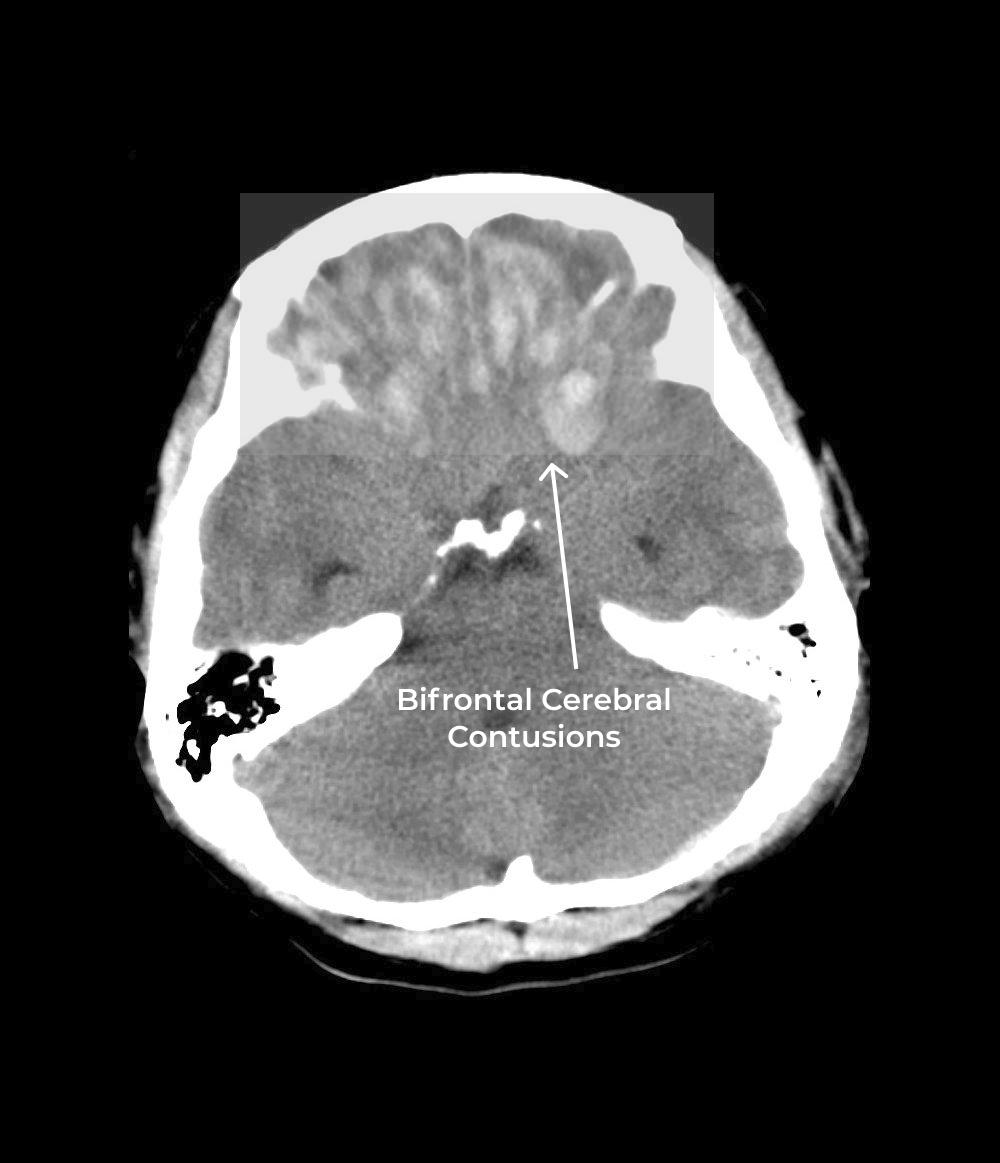
Hemorrhagic contusion are common to see in significant head injury. Most contusions represent the brain coming to a sudden stop against the inner surface of the skull (contrecoup) accentuated by the natural contours of the skull.
Contusions vary in size and can appear as small petechial foci of hyperdensity/hemorrhages involving the grey matter and subcortical white matter or large cortical/subcortical bleed.
Key Findings
Midline Shift
Midline of the brain is curved due to pressure build up inside brain either due to swelling or bleeding.

Caused due to following:
- extra-axial collection causing mass effect
- parenchymal tumor causing mass effect
- stroke with associated edema causing mass effect
Mass Effect
Mass effect describes what happens around a tumor in the brain. It may be caused by:
- tumors
- cerebral abscess
- infarction and associated edema
- hemorrhage
Hydrocephalus
It describes the situation where the intracranial ventricular system is enlarged because of increased pressure. It may be caused by:
- obstruction of CSF flow.
- altered CSF dynamics.